An inflammatory liver disease of unknown cause characterized by suppressor T-cell defects with autoantibodies directed against hepatocyte surface antigens. AIH predominantly affects young or middle-aged women (bimodal, i.e 10–30yrs or >40yrs old).
Presentation:
Up to 40% present with acute hepatitis and signs of autoimmune disease such as fever, malaise, urticarial rash, polyarthritis. The remainder present with gradual jaundice or are asymptomatic and diagnosed incidentally with signs of chronic liver disease.
Pathogenesis:
Involves the combination of genetic predisposition and environmental triggers.
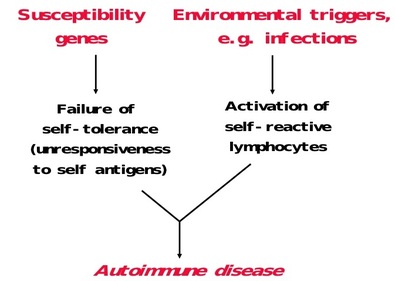
Genetic predisposition
- Genetic susceptibility to developing autoimmune hepatitis has been associated with the HLA haplotypes B8, B14, DR3, DR4, and Dw3
- C4A gene deletions are associated with the development of autoimmune hepatitis
- Viruses:
- Drugs
Investigations:
- CBC (pancytopenia secondary to hyperspleenism)
- Bilirubin, ALT, AST, ALP (usually all raised)
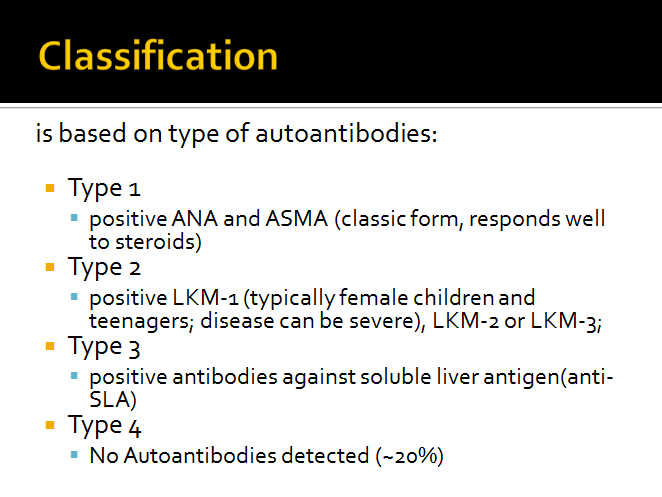
- Autoantibodies
- ANA
- ASMA
- Anti-LKM
- Anti – SLA
- Serum IGg Levels
- Liver Biopsy
- Investigations to rule out other causes of CLD
- AntiHCV, HBsAg
Liver Biopsy
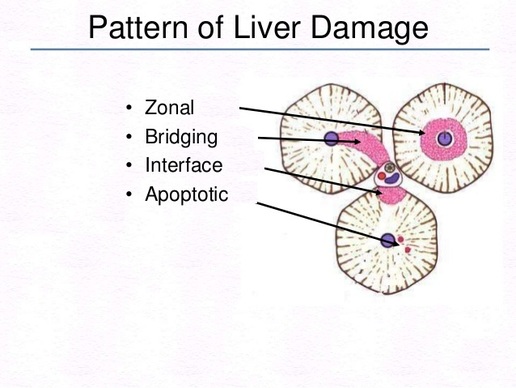
“Piecemeal necrosis” or interface hepatitis with lobular or panacinar inflammation (lymphocytic and plasmacytic infiltration) are the histologic hallmarks of the disease.
It refers specifically to a loss and degeneration of (limiting plate) hepatocytes at the lobular-portal-interface, producing a moth-eaten irregular appearance.
It refers specifically to a loss and degeneration of (limiting plate) hepatocytes at the lobular-portal-interface, producing a moth-eaten irregular appearance.
- In Autoimmune Hepatitis Bridging or interface hepatitis occurs
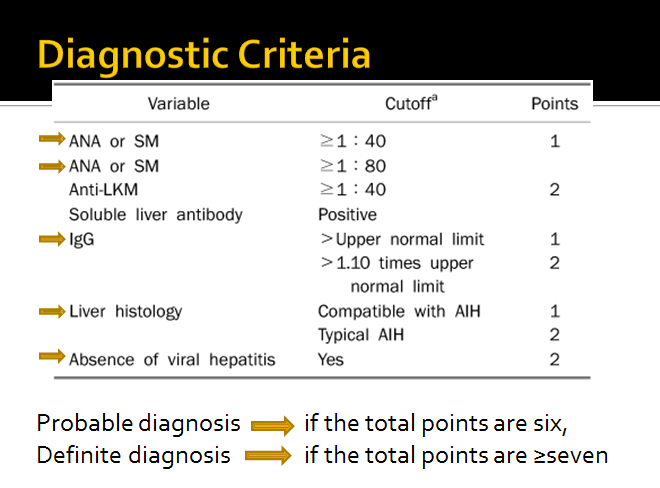
How to Diagnose:
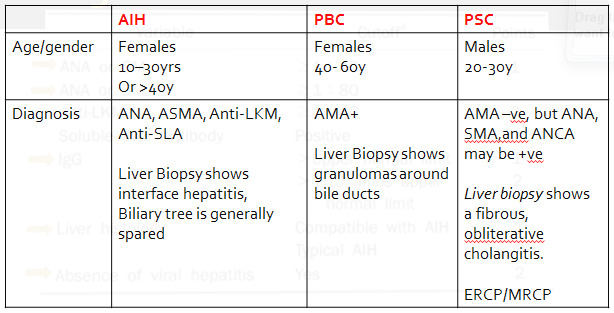
Differential Diagnosis
AIH is a diagnosis of exclusion; Viral and drug-induced causes must be ruled out.
- Primary Biliary Cirhosis
- Primary Sclerosing Cholangitis
- Chronic Viral Hepatitis
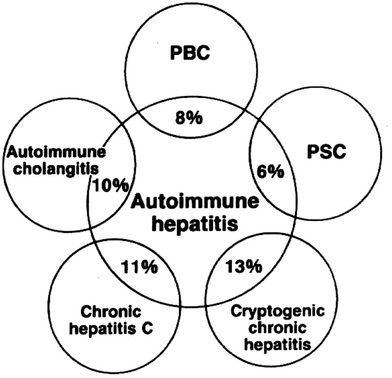
- Overlap Syndrome
- AIH plus PBC, AIH plus PSC
Overlap Syndromes:
Associated Conditions
- Type I diabetes mellitus
- Thyroiditis
- Idiopathic thrombocytopenic purpura
- Ulcerative colitis
- Rheumatoid arthritis
- Primary biliary cirrhosis and primary sclerosing cholangitis occasionally overlap with AIH
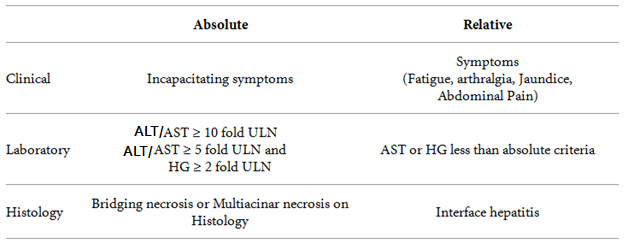
Indications for treatment
Treatment
Immunosuppressant therapy
First Line Drugs:
Liver transplantation
First Line Drugs:
- Prednisolone
- Azathioprine
- Cyclosporine
- Tacrolimus
- Mycophenolate Mofetil
Liver transplantation
Prednisolone monotherapy and prednisolone in combination with Azathioprine are equally effective in induction and maintenance of remission
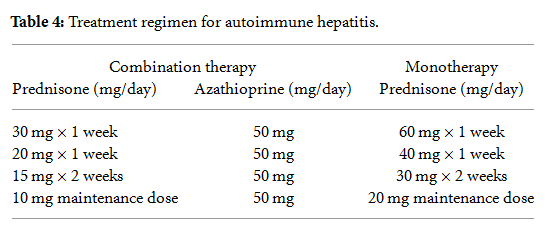
Combination therapy is preferred in:
Second Line drugs are considered if there is no improvement in clinical, lab and histological features after 6 weeks of therapy
- Osteoporosis, Diabetes, HTN, Obesity, Acne, Depression
- Cytopenias
- Pregnancy
Second Line drugs are considered if there is no improvement in clinical, lab and histological features after 6 weeks of therapy
Endpoints of treatment
Primary End Point
Secondary End Point
Final Goal
- Normalization of ALT
Secondary End Point
- Normalization of Histologic activity
Final Goal
- To achieve sustained remission without need of drug therapy or at lowest dose possible, and maintaining the hepatic reserve
Follow Up:
ALT and IgG level may be followed two weekly on a regular basis as a marker of disease responsiveness to therapy.
Reference:
AASLD Guidelines
 RSS Feed
RSS Feed