Carcinoid Syndrome:
Carcinoid syndrome refers to the array of symptoms that occur secondary to carcinoid tumors. Carcinoid syndrome occurs in approximately 5% of carcinoid tumors. These are diverse group of tumours of neural crest (enterochromaffin cells) origin, by definition capable of producing 5HT (Serotonin). Etiology of carcinoid tumors is not known, but genetic abnormalities are suspected. Reported chromosomal abnormalities include changes in chromosomes, such as numerical imbalances. Manifest when vasoactive substances from the tumors enter the systemic circulation escaping hepatic degradation.
Main vasoactive substances include:
If the primary tumor is from the GI tract (hence releasing serotonin into the hepatic portal circulation), carcinoid syndrome generally does not occur until the disease is so advanced that it overwhelms the liver's ability to metabolize the released serotonin.
Main vasoactive substances include:
- Serotonin
- Kallikrein (catalyzes the conversion of kininogen to bradykinin which is a powerful vasodilator and bronchoconstrictor)
- Histamine
If the primary tumor is from the GI tract (hence releasing serotonin into the hepatic portal circulation), carcinoid syndrome generally does not occur until the disease is so advanced that it overwhelms the liver's ability to metabolize the released serotonin.
Common Sites:
- Appendix (45%)
- ileum (30%)
- Rectum (20%)
- Other parts of GI tract, ovary, testis, and bronchi (5%)
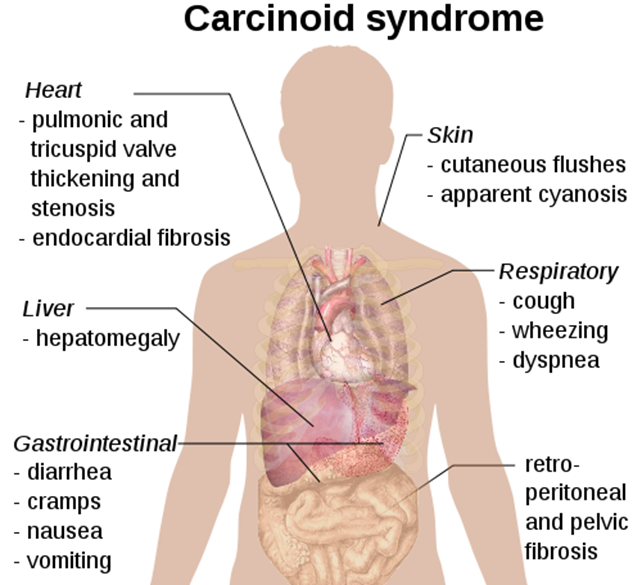
Signs and symptoms
Signs and symptoms vary greatly and depend on the tumor location and size as well as on the presence of metastases. It may present as
- Incidental Finding
- tumor-related symptoms
- carcinoid syndrome
- GI tumors can cause appendicitis, intussusception, or obstruction.
- Hepatic metastases may cause RUQ pain
- Pellagra
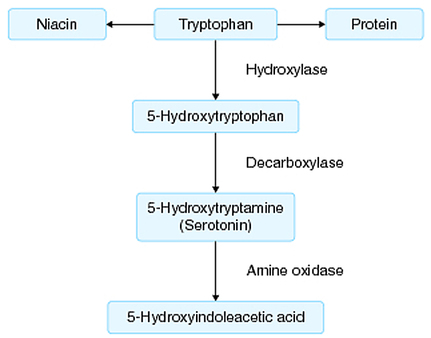
Serotonin Metabolism
Diagnosis:
1. Biochemical Markers:
5-hydroxy-indole-acetic acid (5-HIAA)
Chromogranin A (CgA)
2. Imaging techniques
Conventional Imaging Modalities (CT, MRI, Ultrasound, Endoscopy) are used to locate tumors. Following scans can be performed to diagnose carcinoid tumors.
Octreoscan
5-hydroxy-indole-acetic acid (5-HIAA)
- End product of serotonin metabolism
- Most useful initial test
- Measured in 24 hour urinary collection
- Patients with carcinoid syndrome usually excrete >25 mg of 5-HIAA per 24 hour
- Sensitivity 75% Specificity 100%
Chromogranin A (CgA)
- Present in wall of synaptic vesicles that store serotonin and glucagons
- Levels correlate with tumour bulk
- Elevated in 85-100% pts with carcinoid tumour
- Sensitivity 67.9% Specificity 85.7%
2. Imaging techniques
Conventional Imaging Modalities (CT, MRI, Ultrasound, Endoscopy) are used to locate tumors. Following scans can be performed to diagnose carcinoid tumors.
Octreoscan
- Initial imaging method for localization of both primary lesions and metastasis
- Indium-111 labelled somatostatin analogues (octreotide ) are used in scintigraphy for detecting tumors expressing somatostatin receptors.
- Detection rates with octreoscan are about 89%, in contrast to other imaging techniques such as CT scan and MRI with detection rates of about 80%
- Used to detect carcinoid and other neuroendocrine tumours
- Uses 123I- or 131I-labelled MIBG
- Useful for tumours which do not have somatostatin receptors
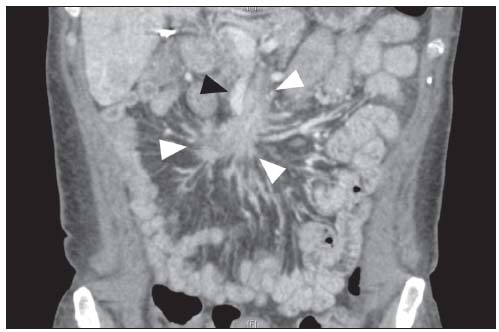
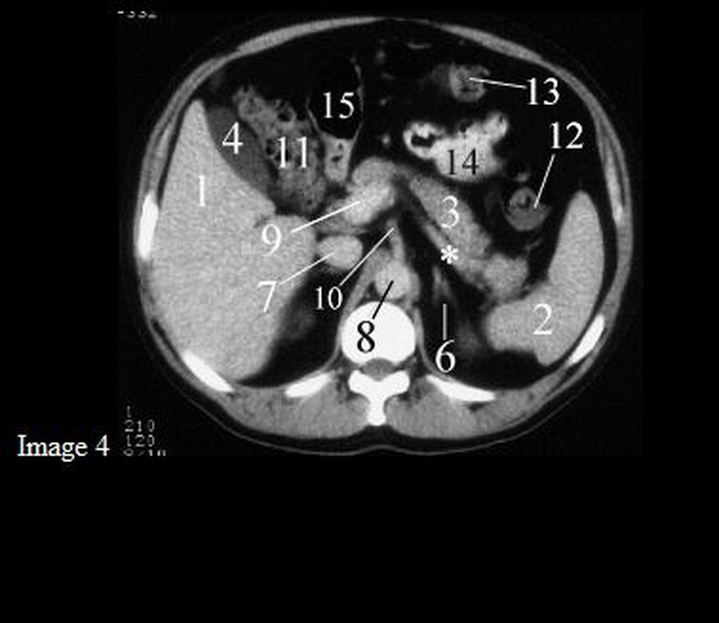
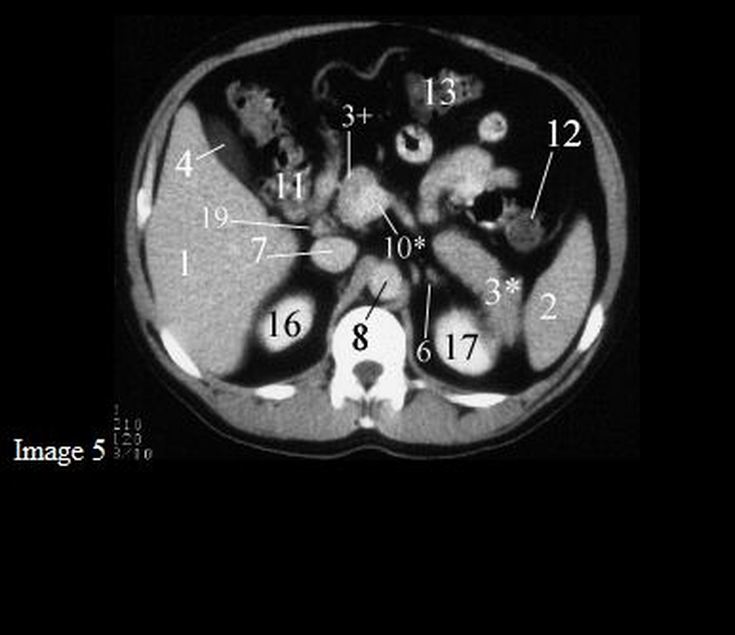
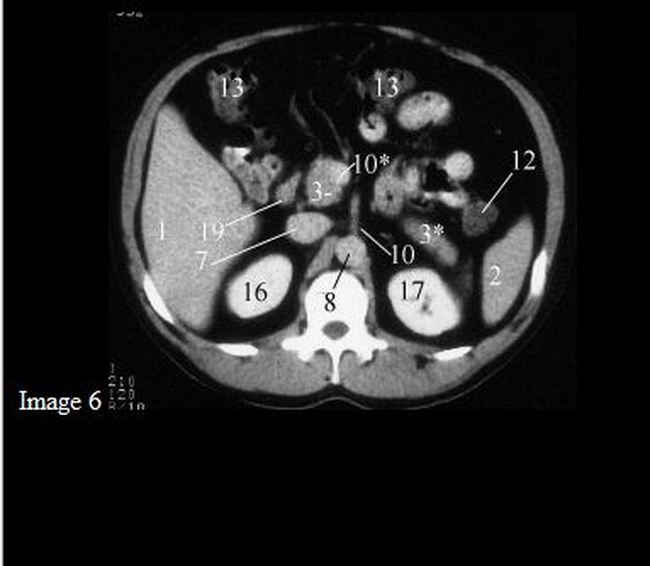
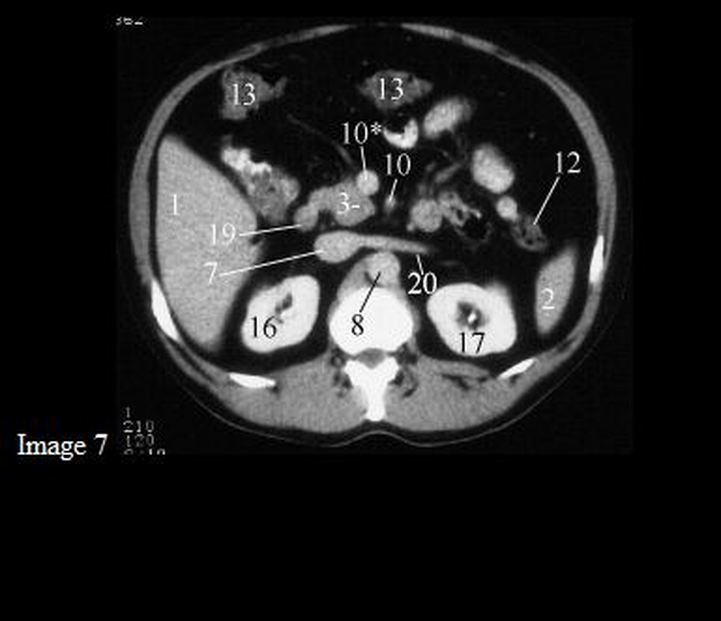
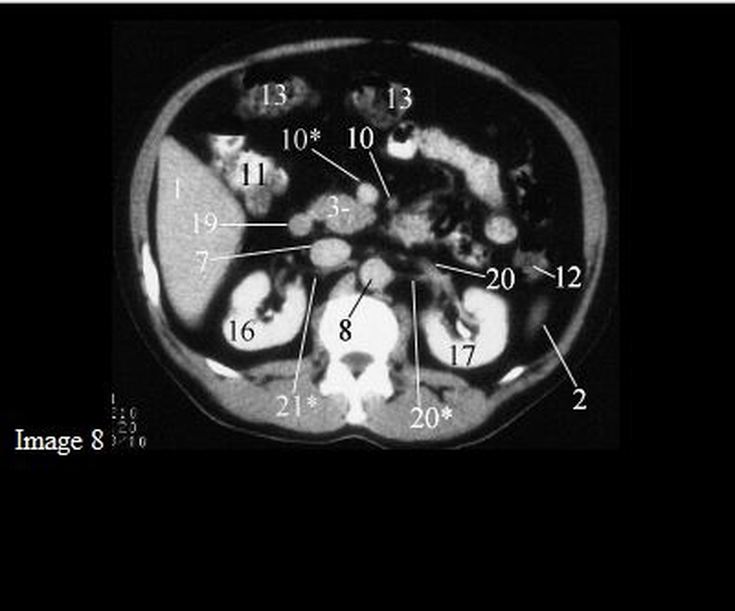
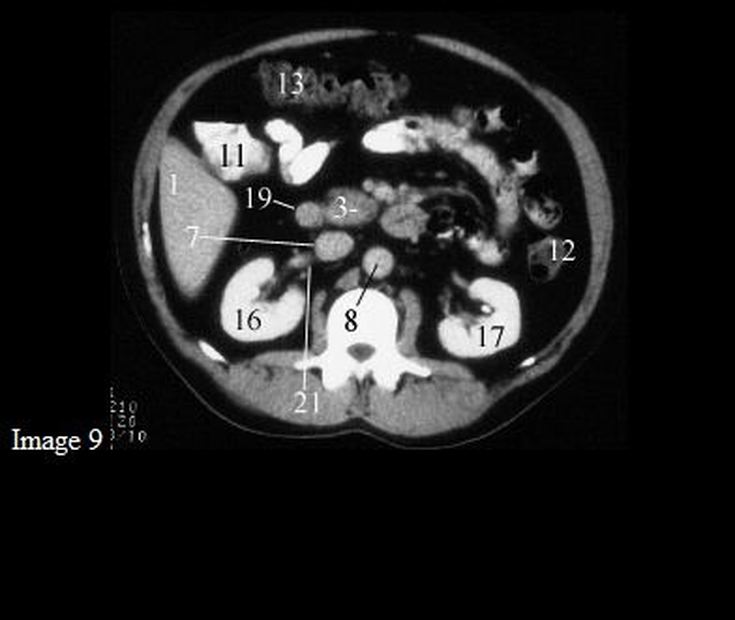
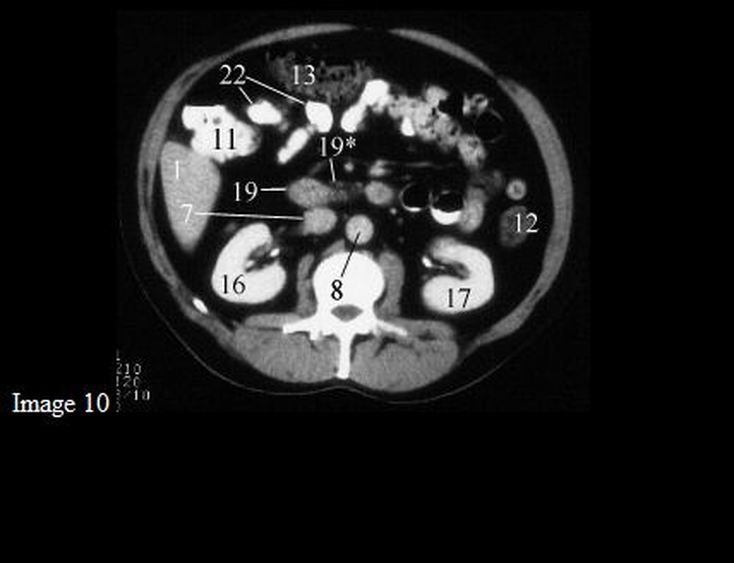
CT scan of a patient with Carcinoid syndrome, a spider-like/crab-like change (Arrow heads) is visible in the mesentery due to the fibrosis from the release of serotonin.
Treatment:
1. For symptomatic relief of carcinoid syndrome
Octreotide (Sandostatin)
3. Chemotherapy (5-FU and doxorubicin)
4. Endovascular chemoembolization, targeted chemotherapy directly delivered to the liver through special catheters used for patients with liver metastases.
Octreotide (Sandostatin)
- somatostatin analogue which decreases the secretion of serotonin by the tumor
- Initial Treatment with solution: 100-600 mcg/day SC divided q6-12hr; may titrate up to 1500 mcg/day for 2 weeks
- Maintenance with Suspension (depot injection): 20 mg IM every 4 weeks
3. Chemotherapy (5-FU and doxorubicin)
4. Endovascular chemoembolization, targeted chemotherapy directly delivered to the liver through special catheters used for patients with liver metastases.



















 RSS Feed
RSS Feed