A 74 year old male, resident of Islamabad presented in our ER witrh Multiple episodes of palpitations and dizziness with a blood pressure of 90/50 mmHg during episodes and a heart rate of 160 to 170 bpm. Comorbids include dyslipidemia and Previous Anterior wall MI, 19 years ago Had PCI to LAD at that time.
On presentation his B.P = 125/80mmHg, Pulse = 85 bpm , Afebrile, R.R = 15/min, Spo2 = 99% at room air. Chest was Clear, audible S1, S2 without any added sound or murmur , JVP wasn’t raised, no pedal edema
Baseline Labs:
◦Na = 138 mEq/L
◦K= 4.1 mEq/L
◦Mg = 2.1 mg/dL
◦Ca = 9.4 mg/dL
◦Cr= 0.9 mg/dL
◦CBC – Normal
◦Cardiac Enzymes - Normal
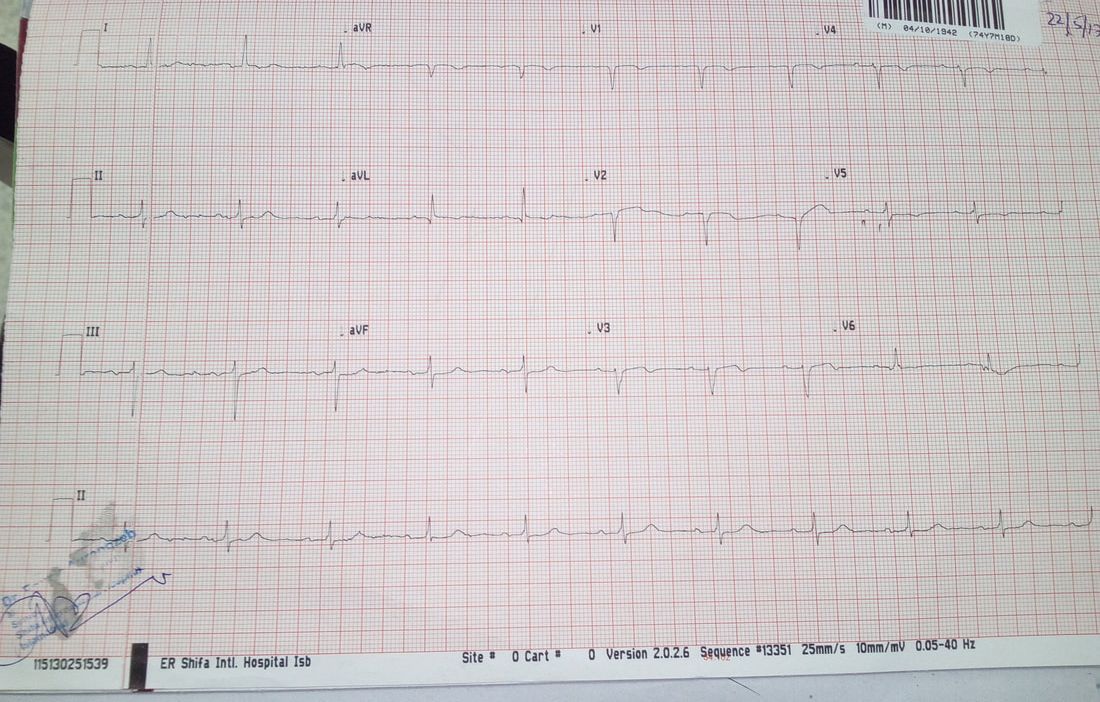
ECG
◦evidence of old anterior wall MI
◦No arrhythmia detected at presentation
On presentation his B.P = 125/80mmHg, Pulse = 85 bpm , Afebrile, R.R = 15/min, Spo2 = 99% at room air. Chest was Clear, audible S1, S2 without any added sound or murmur , JVP wasn’t raised, no pedal edema
Baseline Labs:
◦Na = 138 mEq/L
◦K= 4.1 mEq/L
◦Mg = 2.1 mg/dL
◦Ca = 9.4 mg/dL
◦Cr= 0.9 mg/dL
◦CBC – Normal
◦Cardiac Enzymes - Normal
ECG
◦evidence of old anterior wall MI
◦No arrhythmia detected at presentation
Echocardiography showed a non-dilated left ventricle of 53/35 mm, with moderate systolic dysfunction. LVEF was 30% with hypokinesia of the septum and anterior wall. See the clip below showing parasternal long axis view.
Coronary Angiography showed a patent stent in the proximal left anterior descending artery with mild Instent restenosis. See the clip below showing left coronary system of this patient.
So 48 hour Holter monitoring was advised which showed:
◦Multiple PVCs
◦Runs of sustained VT
◦Multiple PVCs
◦Runs of sustained VT
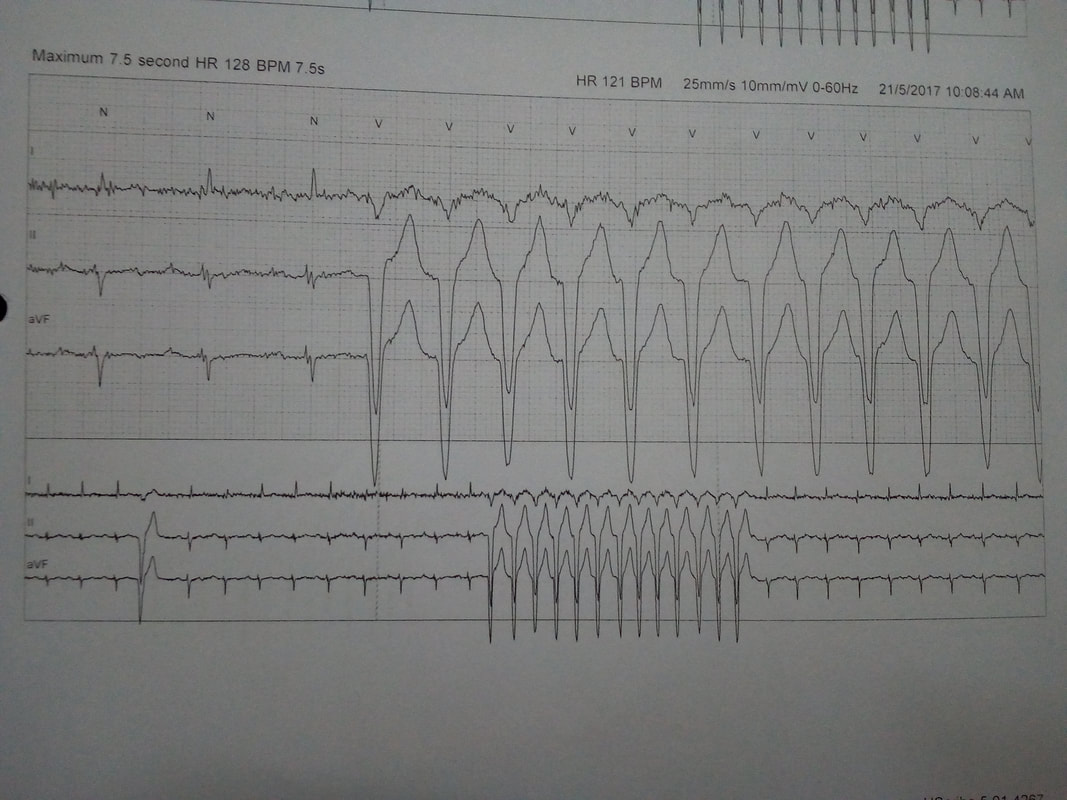
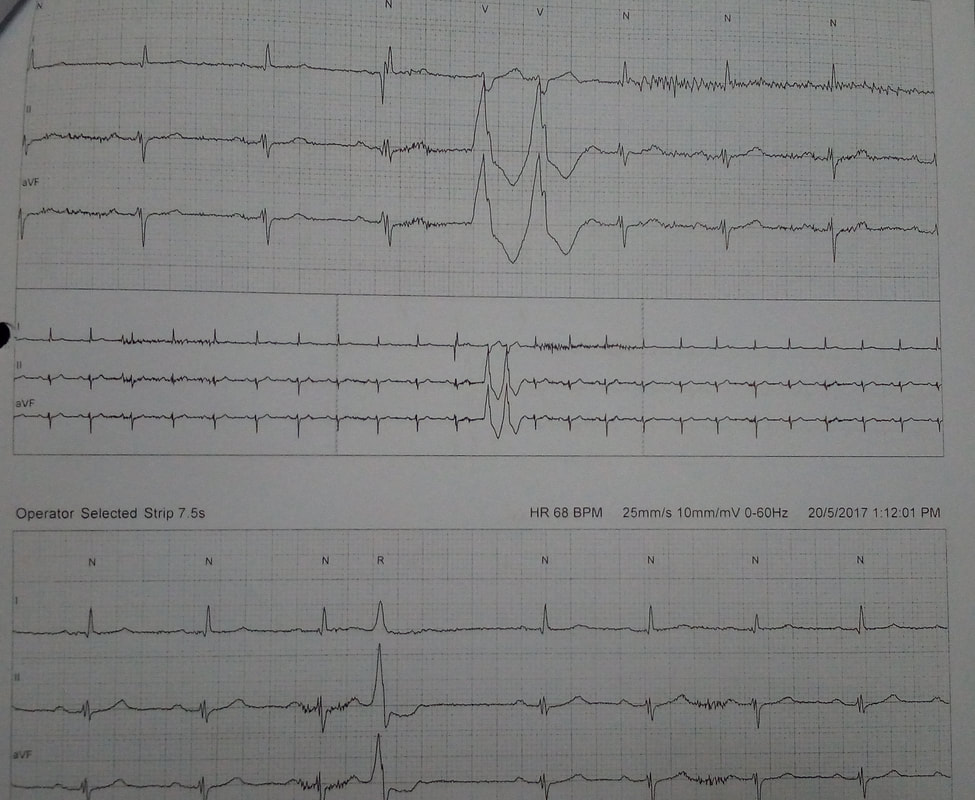
So it was a typical case of Post MI VT/ Scar related VT. In view of symptomatic VT with depressed LV systolic function, excluding acute ischemia he was managed with maximal medical therapy and implantable cardioverter defibrillator (ICD).
Guidelines:
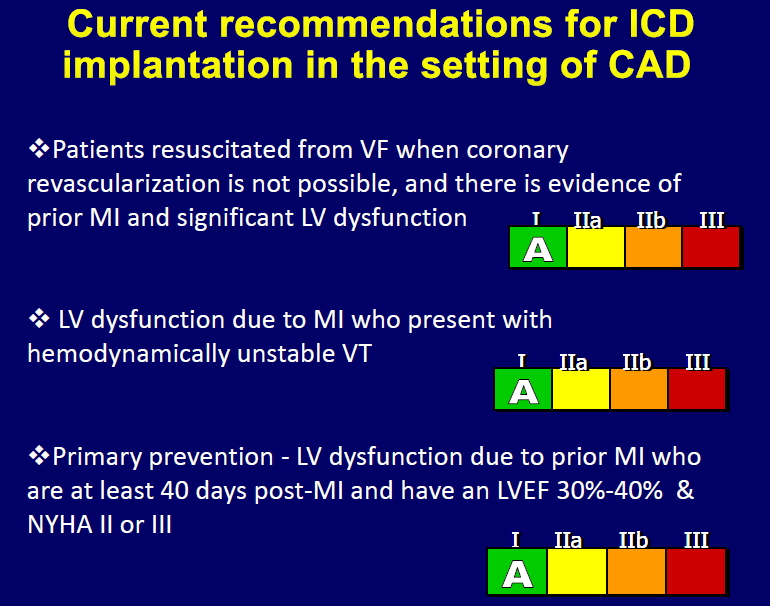
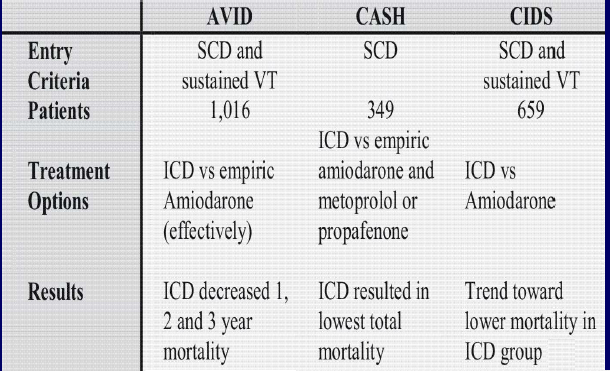
Landmark trials for ICD implantation in post MI VT
 RSS Feed
RSS Feed