Zika virus is a member of the virus family Flaviviridae and the genus Flavivirus, transmitted by daytime-active Aedes mosquitoes, such as A. aegypti and A. albopictus. Its name comes from the Zika Forest of Uganda, where the virus was first isolated in 1947. Below is the documentary video about this virus.
|
- positive Hoffmann’s reflex reflects presence of an upper motor neuron lesion from spinal cord compression;
- is elicited by flipping either the volar or dorsal surfaces of the middle finger and observing the reflexcontration of the thumb and index finger; - positioning the neck in extension (sometimes flexion) may worsen the reflex; - at or above the level of compression, upper extremity should be diminished or absent due to nerve root compression; - in the report by Sung and Wang (2001), asymptomatic patients with a positive Hoffmann’s reflex were prospectively studied with cervical radiographs and magnetic resonance imaging; - to determine a relationship between a positive Hoffmann’s reflex and cervical pathology in asymptomatic patients and to evaluate if further work-up was necessary in this patient population; - 16 patients without cervical pain or radiculopathy and a positive Hoffmann’s reflex were prospectively studied with cervical radiographs and magnetic resonance imaging; - all 16 patients were asymptomatic; - 14 patients (87.5%) demonstrated spondylosis on cervical radiographs; - MRI showed pathologic findings in all 16 patients; - 15 patients (94%) had cervical involvement with cord compression from a herniated nucleus pulposus; - remaining patient had a T5-T6 thoracic disc with resultant compression Key: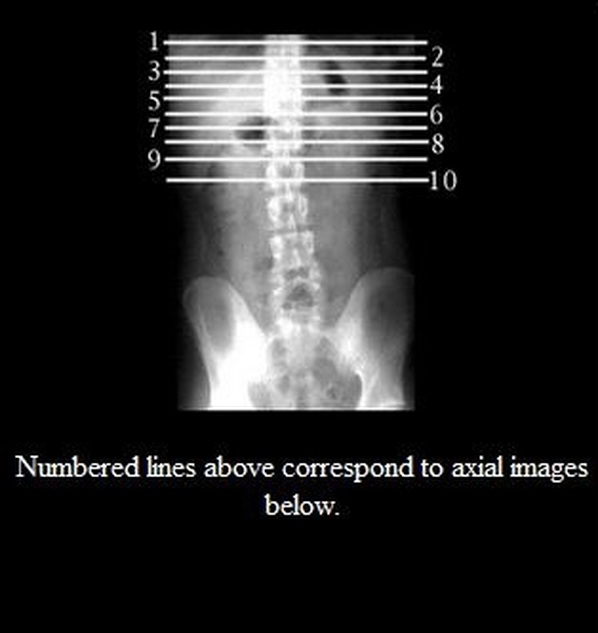 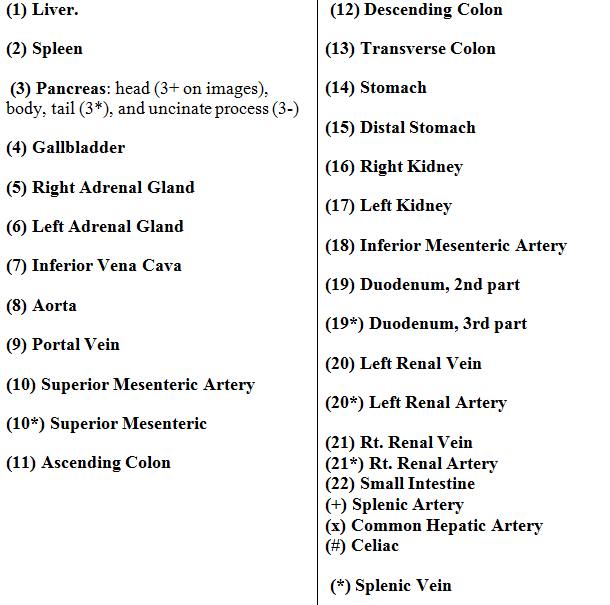 Identification of Basic Structures on Abdominal CT Scan: (1) Liver. (2) Spleen (3) Pancreas: head (3+ on images), body, tail (3*), and uncinate process (3-) (4) Gallbladder (5) Right Adrenal Gland (6) Left Adrenal Gland (7) Inferior Vena Cava (8) Aorta (9) Portal Vein (10) Superior Mesenteric Artery (10*) Superior Mesenteric (11) Ascending Colon (12) Descending Colon (13) Transverse Colon (14) Stomach (15) Distal Stomach (16) Right Kidney (17) Left Kidney (18) Inferior Mesenteric Artery (19) Duodenum, 2nd part (19*) Duodenum, 3rd part (20) Left Renal Vein (20*) Left Renal Artery (21) Rt. Renal Vein (21*) Rt. Renal Artery (22) Small Intestine (+) Splenic Artery (x) Common Hepatic Artery (#) Celiac (*) Splenic Vein 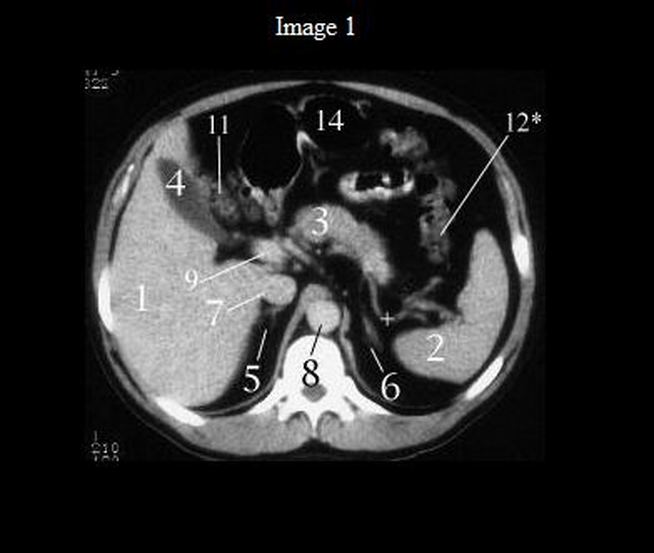 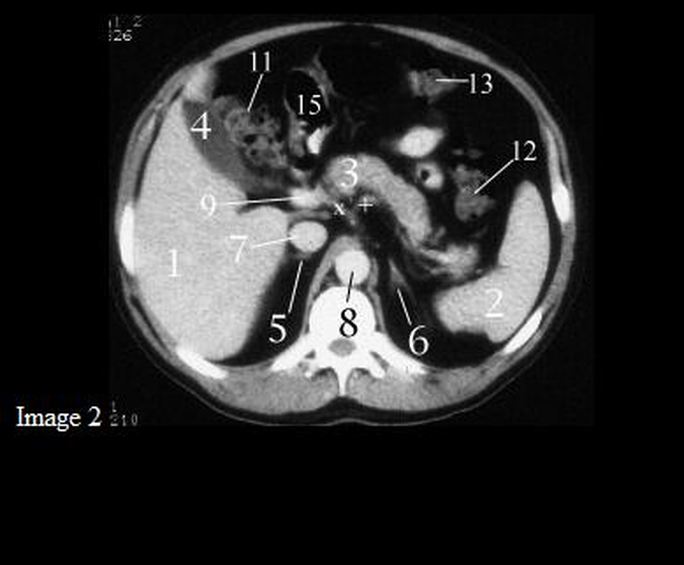 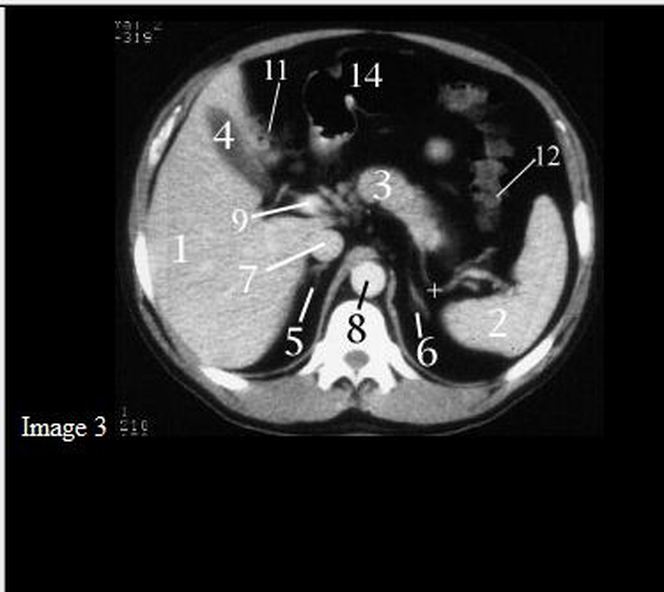 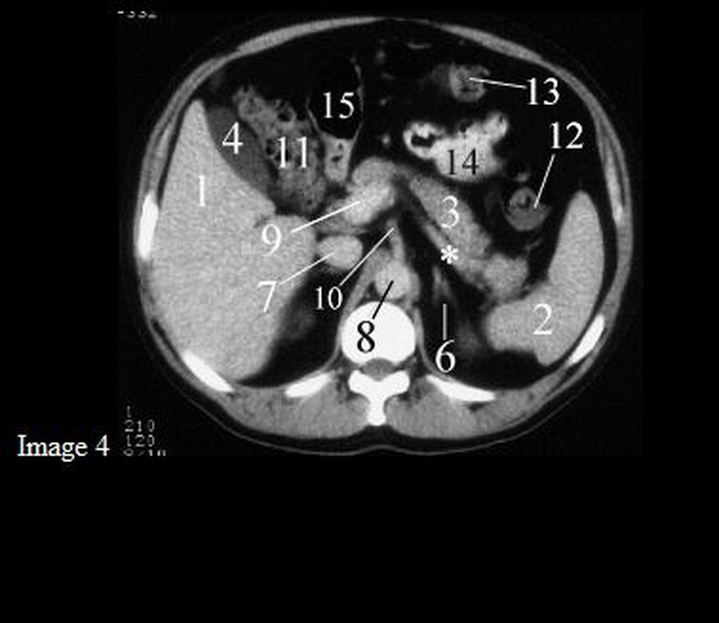 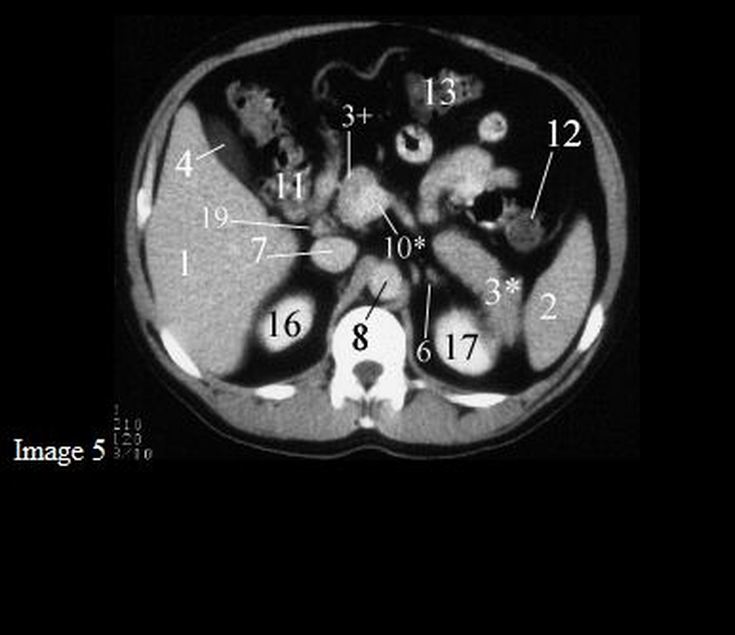 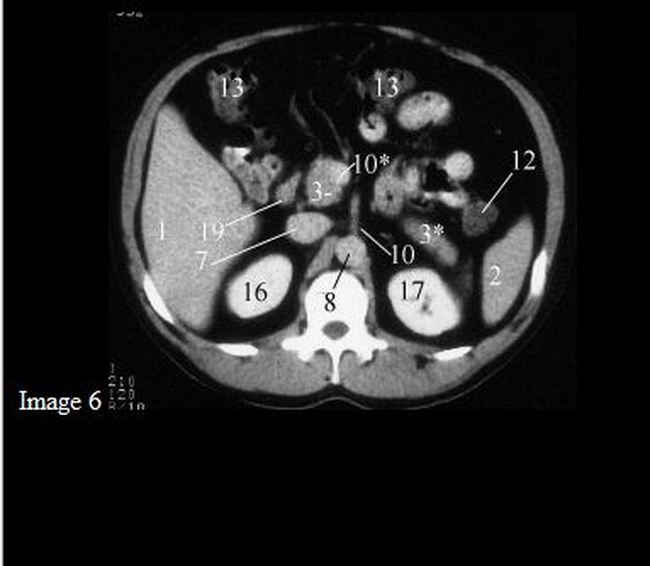 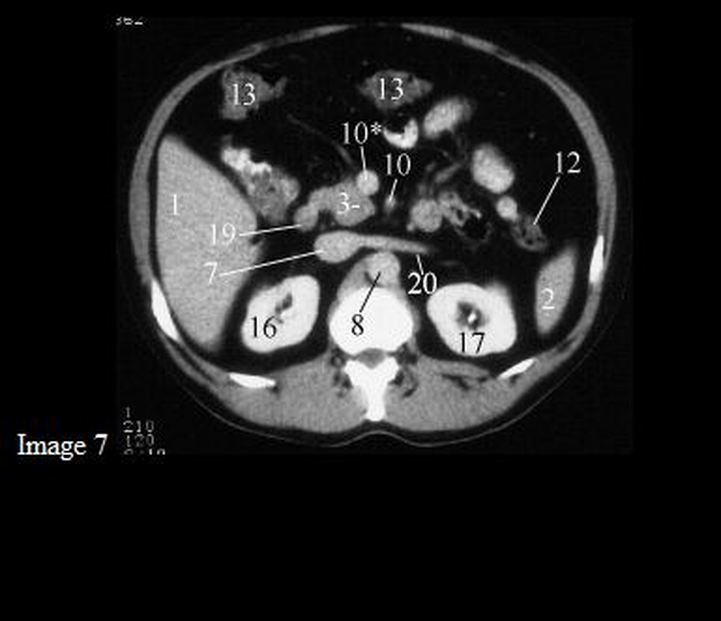 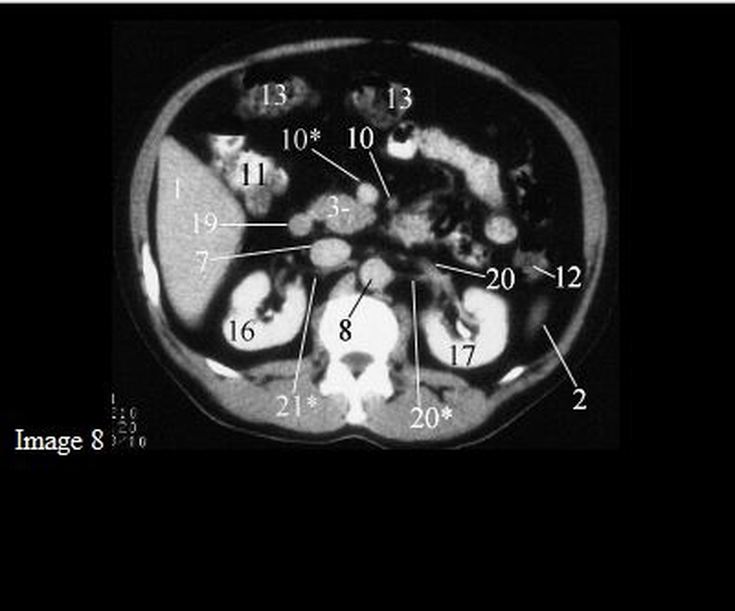 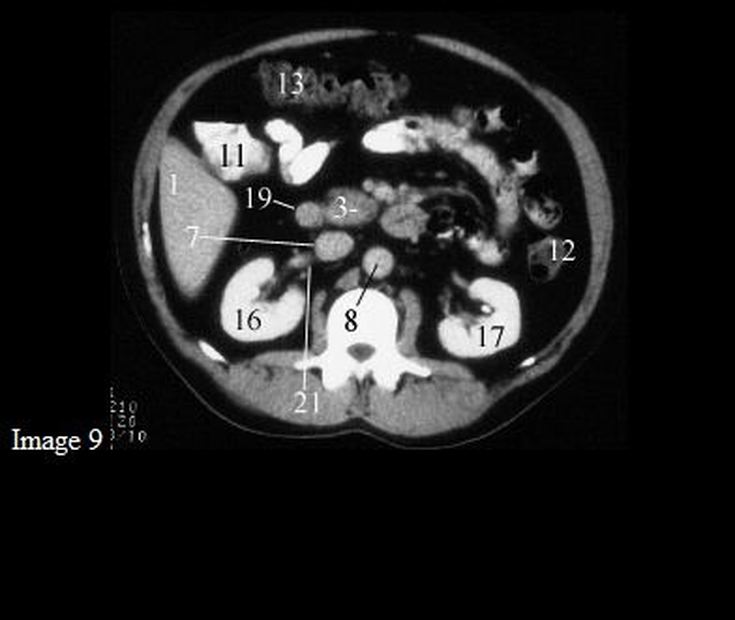 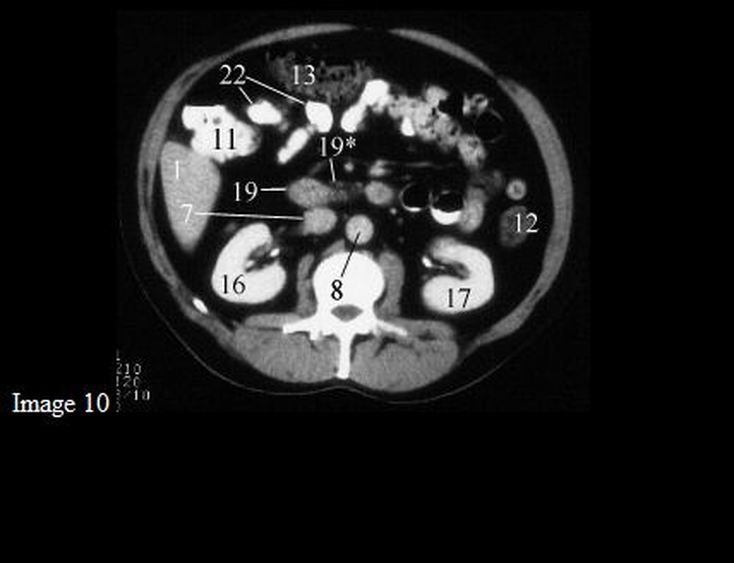  Introduction:There are three types of influenza viruses: A, B and C. Human influenza A and B viruses cause seasonal epidemics of disease almost every winter. The emergence of a new and very different influenza virus to infect people can cause an influenza pandemic. Influenza type C infections cause a mild respiratory illness and are not thought to cause epidemics. Influenza A viruses are divided into subtypes based on two proteins on the surface of the virus: the hemagglutinin (H) and the neuraminidase (N). There are 18 different hemagglutinin subtypes and 11 different neuraminidase subtypes. (H1 through H18 and N1 through N11 respectively.) Influenza A viruses can be further broken down into different strains. Current subtypes of influenza A viruses found in people are influenza A (H1N1) and influenza A (H3N2) viruses. In the spring of 2009, a new influenza A (H1N1) virus (2009 H1N1 Flu) emerged to cause illness in people. This virus was very different from the human influenza A (H1N1) viruses circulating at that time. The new virus caused the first influenza pandemic in more than 40 years. That virus (often called “2009 H1N1”) has now replaced the H1N1 virus that was previously circulating in humans. Influenza B viruses are not divided into subtypes, but can be further broken down into lineages and strains. Currently circulating influenza B viruses belong to one of two lineages: B/Yamagata and B/Victoria. There is an internationally accepted naming convention for influenza viruses. This convention was accepted by WHO in 1979 and published in February 1980 in the Bulletin of the World Health Organization, 58(4):585-591 (1980) . The approach uses the following components:
Signs and symptoms:The symptoms of H1N1 flu are similar to those of other influenzas, and may include fever, cough (typically a "dry cough"), headache, muscle or joint pain, sore throat, chills, fatigue, and runny nose. Diarrhea, vomiting, and neurological problems have also been reported in some cases. People at higher risk of serious complications include those aged over 65, children younger than 5, children with neurodevelopmental conditions, pregnant women (especially during the third trimester), and those of any age with underlying medical conditions, such as asthma, diabetes, obesity, heart disease, or a weakened immune system (e.g., taking immunosuppressive medications or infected with HIV). Severe cases:The World Health Organization reports that the clinical picture in severe cases is strikingly different from the disease pattern seen during epidemics of seasonal influenza. While people with certain underlying medical conditions are known to be at increased risk, many severe cases occur in previously healthy people. In severe cases, patients generally begin to deteriorate around three to five days after symptom onset. Deterioration is rapid, with many patients progressing to respiratory failure within 24 hours, requiring immediate admission to an intensive care unit. Upon admission, most patients need immediate respiratory support with mechanical ventilation. A November 2009 CDC recommendation stated that the following constitute "emergency warning signs" and advised seeking immediate care if a person experiences any one of these signs: In adults:
In children:
Transmission:Spread of the H1N1 virus is thought to occur in the same way that seasonal flu spreads. Flu viruses are spread mainly from person to person through coughing or sneezing by people with influenza. Sometimes people may become infected by touching something – such as a surface or object – with flu viruses on it and then touching their face. "Avoid touching your eyes, nose or mouth. Germs spread this way". The basic reproduction number (the average number of other individuals whom each infected individual will infect, in a population which has no immunity to the disease) for the 2009 novel H1N1 is estimated to be 1.75. A December 2009 study found that the transmissibility of the H1N1 influenza virus in households is lower than that seen in past pandemics. Most transmissions occur soon before or after the onset of symptoms. The H1N1 virus has been transmitted to animals, including swine, turkeys, ferrets, household cats, at least one dog and a cheetah Diagnosis:Confirmed diagnosis of pandemic H1N1 flu requires testing of a nasopharyngeal, nasal or oropharyngeal tissue swab from the patient. Real-time RT-PCR is the recommended test as others are unable to differentiate between pandemic H1N1 and regular seasonal flu.However, most people with flu symptoms do not need a test for pandemic H1N1 flu specifically, because the test results usually do not affect the recommended course of treatment.The U.S. CDC recommend testing only for people who are hospitalized with suspected flu, pregnant women and people with weakened immune systems. For the mere diagnosis of influenza and not pandemic H1N1 flu specifically, more widely available tests include rapid influenza diagnostic tests (RIDT), which yield results in about 30 minutes, and direct and indirect immunofluorescence assays (DFA and IFA), which take 2–4 hours. Due to the high rate of RIDT false negatives, the CDC advises that patients with illnesses compatible with novel influenza A (H1N1) virus infection but with negative RIDT results should be treated empirically based on the level of clinical suspicion, underlying medical conditions, severity of illness and risk for complications, and if a more definitive determination of infection with influenza virus is required, testing with rRT-PCR or virus isolation should be performed. How the Flu Virus Can Change: “Drift” and “Shift”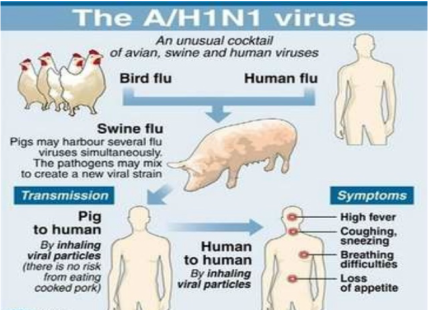 Influenza viruses are constantly changing. They can change in two different ways. One way they change is called “antigenic drift.” These are small changes in the genes of influenza viruses that happen continually over time as the virus replicates. These small genetic changes usually produce viruses that are pretty closely related to one another, which can be illustrated by their location close together on a phylogenetic tree. Viruses that are closely related to each other usually share the same antigenic properties and an immune system exposed to an similar virus will usually recognize it and respond. (This is sometimes called cross-protection.) But these small genetic changes can accumulate over time and result in viruses that are antigenically different (further away on the phylogenetic tree). When this happens, the body’s immune system may not recognize those viruses. This process works as follows: a person infected with a particular flu virus develops antibody against that virus. As antigenic changes accumulate, the antibodies created against the older viruses no longer recognize the “newer” virus, and the person can get sick again. Genetic changes that result in a virus with different antigenic properties is the main reason why people can get the flu more than one time. This is also why the flu vaccine composition must be reviewed each year, and updated as needed to keep up with evolving viruses. The other type of change is called “antigenic shift.” Antigenic shift is an abrupt, major change in the influenza A viruses, resulting in new hemagglutinin and/or new hemagglutinin and neuraminidase proteins in influenza viruses that infect humans. Shift results in a new influenza A subtype or a virus with a hemagglutinin or a hemagglutinin and neuraminidase combination that has emerged from an animal population that is so different from the same subtype in humans that most people do not have immunity to the new (e.g. novel) virus. Such a “shift” occurred in the spring of 2009, when an H1N1 virus with a new combination of genes emerged to infect people and quickly spread, causing a pandemic. When shift happens, most people have little or no protection against the new virus. While influenza viruses are changing by antigenic drift all the time, antigenic shift happens only occasionally. Type A viruses undergo both kinds of changes; influenza type B viruses change only by the more gradual process of antigenic drift. References:
|
Blog Authors:
|

 RSS Feed
RSS Feed